Download this episode
School of Biological Sciences Associate Professor Lewis Wheaton uses his Cognitive Motor Control Lab to research the neurological processes involved when people cope with the loss of a limb, a stroke, or a traumatic brain injury that can impact motor skills.
(Upbeat music)
Renay San Miguel: Hello and welcome to ScienceMatters, the podcast of the Georgia Tech College of Sciences. I’m Renay San Miguel.
01:18 Best Years Of Our Lives
“This is when I know I’m helpless, my hands are down there on the bed, I can’t put them on again without calling to somebody for help, I can’t smoke a cigarette or read a book, if that door should blow shut I can’t open it or get out of this room, I’m as dependent as a baby that doesn’t know how to get anything except cry for it. Well, now you know, Wilma, now you have an idea of what it is. I guess you don’t know what to say.”
“I know what to say Homer, I love you and I’m never going to leave you, never.”
(Music swells)
RENAY:
We’re not crying, you’re crying.
That is a key, emotional scene from the 1946 Best Picture winner, The Best Years of Our Lives. The actor playing the returning World War II veteran is Harold Russell, a real-life vet who lost his hands in a Navy training accident.
After all these decades, the movie remains one of the most vivid cinematic depictions of life after war for those who fought, and especially for those who came home forever changed.
Lewis Wheaton in lab:
00:06 “We’re going to put this device on you that is going to sort of making you feel like you have to get used to using a prosthetic limb.”
RENAY:
Another thing that hasn’t changed after all these years, and all the scientific knowledge gained in that time, is that those who suffer the loss of a limb still have to learn how to adapt.
Lewis Wheaton, associate professor in the School of Biological Sciences, wants to know more about how people make those adjustments to major changes in their motor skills. If he learns more, he may be able to make it easier to adapt, and maybe make better prosthetics along the way.
That’s why he’s here working with research team members in the Cognitive Motor Control Lab, where he serves as director.
Team member in lab: 01:07:16
“And around your other arm, we’re gonna give you the harness that actually helps you control the device, so I’ll let you try to figure out how to exactly open and close it.”
RENAY:
One of his students is trying on what Wheaton calls an entry-level prosthesis, a right-handed hook that’s controlled mostly by the left shoulder thanks to cables and pulleys. She’s doing it to get an idea of what it’s like to use a prosthetic device.
The student, Christina, then tries to throw Velcro balls at a target with the prosthetic device.
Wheaton lab nat sound:
Renay San Miguel: You looked like you had to use more muscle.
Christina: It’s definitely an adjustment.
Renay: I would think so. Can I try that?
RENAY:
Then it’s my turn to fit my right arm in the device.
Renay nat sound: “Did you say that this was the standard prosthesis for…”
Wheaton: “Yes this type of the design is really the entry-level prosthetics that most people would get. It’s body-powered, so it’s a harness that controls the opening and closing of this with cable support.”
RENAY:
After a rough start, I finally manage to throw some Velcro balls on the target. Then I’m asked to unlock a lock, pull out the key, and lock things back up.
Renay nat sound: “So unlock it, and I have to yank that bad boy out of there.”
Wheaton: “Right.”
Renay: “It’s not coming.” (Laughter).
RENAY:
I can, of course, remove the device and get my right hand back. Imagine the frustration of a new amputee trying what came naturally before, only to find that simple tasks are now struggles.
Wheaton’s research hopes to help smooth out those struggles.
Whether through traumatic injuries resulting in the loss of a limb, or through strokes or other brain injuries that can take a patient back to square one, Wheaton is out to better understand the neurological processes involved, so that those people can win back their independence.
He’s also learning more about what happens in our brains when we intend to do something, and what happens when we act on those intentions.
03:15 Lewis Wheaton: So the goal of the research of my lab really is to understand the interaction between these two domains that are usually thought of as separate, right? One is cognition, one is motor control, and to understand how those two sub-domains are so important and key to unlocking and helping to support the needs of people and how people think, how people function, how people behave, whether they are you know people that are perfectly healthy and have sound limbs and on and on and on, all the way to people with neural injury and peripheral injuries. How those two sub-domains function together as a unique entity is of critical concern to us.
MUSIC
Forrest Gump 25:04
“Lieutenant Dan.”
“Hello Forrest.”
“You got new legs. New legs!”
“Yeah, I got new legs. Custom-made titanium alloy. It’s what they use on the space shuttle.”
“Magic legs.”
RENAY:
For Wheaton, the magic happens in the mind-body connection.
Earlier, he said his lab’s mission was to learn everything about cognition, and motor control. Cognition implies thought or intent, motor control is the action.
But Wheaton peels away other layers of that connection.
0:04:39
Lewis Wheaton: For me I think of it as kind of intersection of three domains, really. There’s the biological aspect of it because you’re dealing, at least in my world, we’re dealing with people and understanding, you know, all these biological aspects of humans. There’s the engineering side, particularly when it comes to prosthetics that I’m very intrigued about. But then there’s the psychology side as well where you’re kind of pulling in, “OK what’s motivating people to move and how they move?” An example that I always give my students is the idea of doing something as simple as reaching for a coffee mug. If you reach for a coffee mug, you will likely reach to that mug differently depending on why you’re reaching for it. If you’re just reaching to move a mug around you’re going to grab it from the top. You’re not going to care because you’re not—your goal is not to drink from it, your goal is just to move it around or something.
Renay San Miguel: Yeah I’m not going to grab it by the handle.
Lewis Wheaton: Yeah, exactly, but if your goal is to drink it, you’re pretty much always going to grab it by the handle or you’re going to grab it by the side. That’s just how you do. Why do you do that? That’s one of the things that we’re continually curious about.
Renay San Miguel: What’s the one surprising thing you have found in your research as to how people or, better yet, our brains, how we adapt to these challenges? What’s the one thing that’s just blown you away?
Lewis Wheaton: So I think of almost two things really that are equally impressive to me. One is the creativity of people. It’s so cool to have people in our studies that are doing daily activities where we’re trying to get them to either behave in daily circumstances or trying to judge behavioral things that they’re observing and the very different impressions they take away from it or the very different strategies they take to move something around. It’s really beautiful, and it speaks to this sort of—while there’s a common humanity there, it speaks to these little differences that we all have in how we approach something.
0:07:42
The other thing that is captivating, and this is something that’s sort of being—is emerging in the research of the lab—is the power of something as simple as the visual system. So we’ve looked at a lot of things from the perspective of how is the brain changing if we look at condition A versus condition B, we’ve looked at how is the body moving differently—moving condition A versus condition B—but one of the things we kind of tripped on, and this is one of my grad students who was curious about this question and we said, “Well, let’s look at what the eyes are doing.” There’s never been a mystery about the fact that the eyes seemingly guide behavior; they guide our intent. You know you tend to look at what you want to grab, things like that. But we started to realize that the visual strategies that people employ when they’re trying to solve problems are so unique. And they differ depending on who you are—if you’re a younger person versus an older person; if you’re somebody that does not have amputations versus somebody that does have an amputation; whether or not you have somebody with a stroke that is in acute phase versus somebody in chronic phase. You’re using the visual system to help guide behavior and you’re always doing it differently. Well, the cool part about that is the eyes aren’t just working by themselves. They’re also working in coordination with the brain. So if for some reason the brain is picking up on differences. They’re helping to align visual system to look for differences, perhaps implicitly, and strategies and things like that that help movement, and then you’re actually using that information to help guide movement. And it’s been so beautiful to see that.
0:09:50
CUT TO LAB
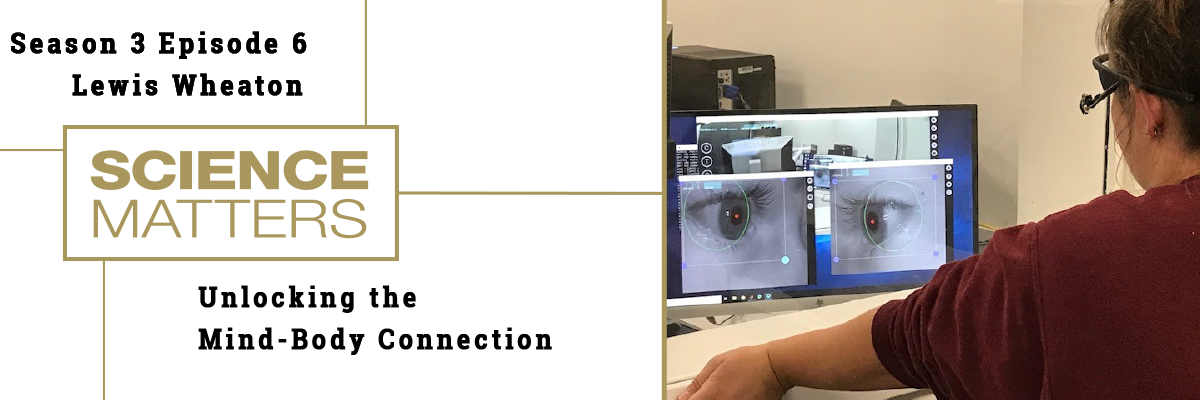
Woman team member 02:45
“These two pupil cameras are on there, and essentially what they’re doing, they’re detecting where your pupils are relative to the world view, so what we actually see on our end is what you’re seeing along with where your pupils are relative to that world view.”
“Go ahead and look straight ahead, follow my finger, I just want to make sure all pupil cameras are detecting your pupils regardless of where your head position is.”
RENAY:
Thanks to the use of tiny cameras on special glasses, Wheaton and his team members are focusing on eye-tracking as a way to help make the rehabilitation process – that is, learning to use a prosthetic device – more efficient. They study what test subjects look at when watching someone with both upper limbs perform a task, versus someone using a device. Those who watch the person with the device are looking more at the parts of the body that power that device – the left upper body, for example, for someone using a right-handed prosthetic device.
Lewis Wheaton: That’s part of one of the approaches we tend to take in the lab is looking at, you know, there are people that come in all the time and they either feel as though they can’t do something or they feel as though—or they’ve adapted to doing it in a way that is so different, but it is perhaps different in a bad way. It’s what we refer to generally as something that’s maladaptive, right? We pick up a maladaptive behavior to compensate for this limitation. And, you know, part of that comes back to the creativity that people individually have, but there’s also that challenge of getting people to understand that they may have a desire to do something, so to speak, in their mind, but they can figure out a way to make it happen, right? So that’s getting from that, you know, having that—the intent of “Here’s what I love to do” to that action where you’re like, “All right! Now I can do it, and here’s exactly how I would do it.” And do it not only in a reducible way, but in a way that won’t cause more harm down the line.
MUSIC
RENAY:
Let’s dig deeper into the intent vs. action process within our brains. Wheaton explains the first time he saw this play itself out. It was during his third year of graduate studies.
0:12:12
Lewis Wheaton: I saw this particular patient who had a stroke, a very small stroke. And the left side of the brain, the parietal lobe, had really no deficits to speak of resulting from the stroke except one problem, one singular problem: When we asked her to do various gestures with her hands, particularly communicative gestures, so something like waving goodbye, “Show me how you’d wave goodbye. Show me a peace sign,” things like that, she could describe it, she could say when she would do it, she couldn’t do it. She could raise her hand, but she couldn’t make her hand move in the way that she needed to make it move. She could explain for like a peace sign, for example, she could explain that she needed to move her thumb down to her palm and that she needed to move her ring finger and her small finger down to leave the first and the middle finger up. She could describe it but she couldn’t do it.
Lewis Wheaton: That to me really captured the difference between intent and action. That particular deficit is referred to as apraxia. It’s a version of apraxia called ideomotor apraxia where you struggle making these gestures though you know what you’re trying to do. But we see this—and it’s not necessarily apraxia—but we see similar things played out in a lot of cases. People with upper limb loss, they’re dealing with prostheses; they know they want to pick up the mug. They can’t quite figure out the strategy to use to pick up the mug with the device, so they just use their sound limb if they have unilateral limb loss. They just default to that in some cases. Some people try different strategies, but it can be hard, it can be difficult. So how to get people maybe a bit better on that continuum saying, “Here’s what I want to do and here’s how I’m going to do it.” Very similar to how, you know, probably most people can. You know, if you ask people to wave goodbye, they can wave goodbye perfectly fine. But seeing those people struggle with something like that is humbling and it’s really remarkable to think about what’s the disconnection between those two systems that keeps the cognitive, perhaps, disconnected from the motor? That keeps the intent separate from the action. That’s what’s really an elegant problem in neuroscience.
Renay San Miguel: What about just natural aging? No injury of any kind, no strokes, people take care of themselves, but the years will have an impact on that connection. Tell me about what you’re learning regarding the aging process and how it impacts motor control?
Lewis Wheaton: Yeah, the aging is really interesting. So a lot of people that I know that study certain of these pathologies, things like stroke or some of the degenerative diseases, will often comment anecdotally, “You know, we’re seeing some things, but we still don’t totally know the substrate of aging and how that relates to this.” So for example, in stroke most of the population that you’re studying tends to be a little older. That’s unfortunately not all that uncommon, but then it makes you think is what you’re seeing augmented by the fact of the aging process? Is the aging process somehow maybe being accelerated because of the neural pathology that you’re having? So there are questions really that revolve around that. We do see though in some of our work, and this is perhaps a bit more anecdotal, but we do see some unique differences in a lot of people that are older versus younger, particularly amongst our amputation population. There are certain—and part of it there’s a theory that people have just sort of generally talked about particularly when it comes to this about the idea of technology. And you think about a upper limb prosthetic for example, if you think of it as a piece of technology, are there people that are more than likely to adopt that technology?
0:17:36
It’s comparable to people that are more than likely to adopt any other form of technology. Does age play a role there? Right? Does age play a role in thinking, “Well, if I’m older, I don’t want to figure out how to use a prosthetic limb. That’s too much effort. I don’t care about that.”
Renay San Miguel: Does your research help pave the way for maybe better prosthetics? I mean the ones that actually maybe in the future or maybe it’s around right now, they actually can plug into your nerve system—nervous system?
Lewis Wheaton: Absolutely. I think you know when we think about the training-based approach, I tend to think of myself as not necessarily caring what type of device it is right now. Take any device: How do you still train people on how to use it? Whatever it is, there’s going to be a learning curve. I would love to be able to take a lot of different devices and suggest is there a way perhaps with an array of devices that we can develop presently right now—whether or not they’re available in the market is a separate question—but with the devices we have right now is there a way that we can perhaps say you know based on your physiology, based on your trained responses, this is the device that’s right for you, right? Or—and additionally, I should say, based on the work that we’re seeing here with motor adaptation and motor learning with this type of device, this suggests that this type of device or this feature of the device is not beneficial that we need to perhaps go with different strategies. There’s the engineering side where we could easily just say, “Whoa, we’ll just rebuild, redevelop,” which is great; which is genius I think. But there’s also the understanding of OK, how would the person use it? How can the person use it? Can the person use it? And if they can’t, no matter how cool it is, maybe we need to pull back on that and take some different approaches. And so that’s where, hopefully, you know, this work looking at these modal learning questions with amputation in particular can help to improve device design, but also maybe help with device selection down the line.
MUSIC
RENAY:
When he was attending college, Lewis Wheaton was more interested in viruses and bacteria than cognitive motor control. But the right instructor pushed him in a new research direction
Lewis Wheaton: Back in undergrad I tripped over a course. I needed—I always tell people classical senior undergrad, I needed a class to graduate, and I ended up taking this class by who I came to find was just a tremendous neuroscientist about brain and behavior, sounded interesting. And he’s a neurologist, he studied brain behavior from a neuropathological point of view. And when I listened to what he talked about in class, it blew my mind. And one of the things that blew my mind was that you can study the brain but have absolutely no idea how it worked. And that was just a jarring feeling but it was cool, and it really sucked me in. From there, really, it was through graduate school, I really developed an attraction of trying to understand how to help people that are undergoing various trauma, whether it’s trauma directly to the brain, whether it is trauma to the periphery like the limbs or something like that. How do people actually, you know, get better? What is keeping people from getting better from the point of view of the brain and how can we, you know, kind of get around that or shape the brain to make people better? And that really just hooked me to be honest, and I still am hooked on that.”
RENAY:
Even with new technologies that could help speed up the rehabilitation process, the return to independence, in many ways, is a journey that starts with small steps.
Renay San Miguel: It sounds to me like the fact that after all of these years of research and science and developments, the brain largely is still a mystery.
Lewis Wheaton: Yeah. Yeah, it’s stunning to think, you know, how many resources are pointed at trying to understand something that takes up, you know, relatively little volume of your body, but it’s so fundamental to everything that we do and just understanding even how two cells really function and then adding neurons to that little network, it just gets more difficult, more complicated. It’s just—it’s a beautiful puzzle, and I think that’s probably what hooks a lot of us neuroscientists in and keeps us there to still want to try to unlock something that we probably won’t do in our lifetime.
MUSIC
RENAY:
We’d like to thank Lewis Wheaton, associate professor in the School of Biological Sciences and director of the Cognitive Motor Control Lab, for sharing his research with us.
Also thanks to Samuel Goldwyn Production, RKO Radio Pictures, and Paramount Pictures.
Siyan Zhou, a former research associate with the School of Psychology, composed our theme music.
If you enjoyed this podcast, please subscribe to ScienceMatters. You’ll find us on Apple Podcasts and Soundcloud.
This is ScienceMatters, the podcast for the Georgia Tech College of Sciences. Thank you for listening.
